MAKE A MEME
View Large Image
| View Original: | Image_from_page_556_of_"Local_and_regional_anesthesia_:_with_chapters_on_spinal,_epidural,_paravertebral,_and_parasacral_analgesia,_and_on_other_applications_of_local_and_regional_anesthesia_to_the_surgery_of_the_eye,_ear,_nose_and_throat,_and_to_dental_p.jpg (756x1184) | |||
| Download: | Original | Medium | Small | Thumb |
| Courtesy of: | www.flickr.com | More Like This | ||
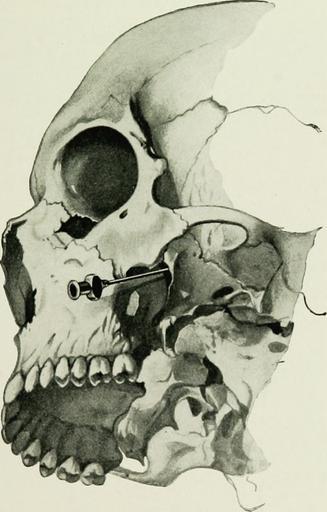
| Keywords: bookid:39002087820487.med.yale.edu bookid39002087820487medyaleedu bookyear:1914 bookyear1914 bookdecade:1910 bookdecade1910 bookcentury:1900 bookcentury1900 bookauthor:allen__carroll_woolsey_1874_ bookauthorallencarrollwoolsey1874 bookauthor:matas__rudolph_1860_1957 bookauthormatasrudolph18601957 booksubject:local_anesthetics booksubjectlocalanesthetics booksubject:anesthetics__local booksubjectanestheticslocal booksubject:anesthesia__local booksubjectanesthesialocal bookpublisher:philadelphia___w_b__saunders_co_ bookpublisherphiladelphiawbsaundersco bookcontributor:yale_university__cushing_whitney_medical_library bookcontributoryaleuniversitycushingwhitneymedicallibrary booksponsor:open_knowledge_commons_and_yale_university__cushing_whitney_medical_library booksponsoropenknowledgecommonsandyaleuniversitycushingwhitneymedicallibrary bookleafnumber:556 bookleafnumber556 bookcollection:medicalheritagelibrary bookcollectionmedicalheritagelibrary bookcollection:cushingwhitneymedicallibrary bookcollectioncushingwhitneymedicallibrary bookcollection:americana bookcollectionamericana drawing surreal monochrome bookid:39002087820487.med.yale.edu bookid39002087820487medyaleedu bookyear:1914 bookyear1914 bookdecade:1910 bookdecade1910 bookcentury:1900 bookcentury1900 bookauthor:allen__carroll_woolsey_1874_ bookauthorallencarrollwoolsey1874 bookauthor:matas__rudolph_1860_1957 bookauthormatasrudolph18601957 booksubject:local_anesthetics booksubjectlocalanesthetics booksubject:anesthetics__local booksubjectanestheticslocal booksubject:anesthesia__local booksubjectanesthesialocal bookpublisher:philadelphia___w_b__saunders_co_ bookpublisherphiladelphiawbsaundersco bookcontributor:yale_university__cushing_whitney_medical_library bookcontributoryaleuniversitycushingwhitneymedicallibrary booksponsor:open_knowledge_commons_and_yale_university__cushing_whitney_medical_library booksponsoropenknowledgecommonsandyaleuniversitycushingwhitneymedicallibrary bookleafnumber:556 bookleafnumber556 bookcollection:medicalheritagelibrary bookcollectionmedicalheritagelibrary bookcollection:cushingwhitneymedicallibrary bookcollectioncushingwhitneymedicallibrary bookcollection:americana bookcollectionamericana drawing surreal monochrome bookid:39002087820487.med.yale.edu bookid39002087820487medyaleedu bookyear:1914 bookyear1914 bookdecade:1910 bookdecade1910 bookcentury:1900 bookcentury1900 bookauthor:allen__carroll_woolsey_1874_ bookauthorallencarrollwoolsey1874 bookauthor:matas__rudolph_1860_1957 bookauthormatasrudolph18601957 booksubject:local_anesthetics booksubjectlocalanesthetics booksubject:anesthetics__local booksubjectanestheticslocal booksubject:anesthesia__local booksubjectanesthesialocal bookpublisher:philadelphia___w_b__saunders_co_ bookpublisherphiladelphiawbsaundersco bookcontributor:yale_university__cushing_whitney_medical_library bookcontributoryaleuniversitycushingwhitneymedicallibrary booksponsor:open_knowledge_commons_and_yale_university__cushing_whitney_medical_library booksponsoropenknowledgecommonsandyaleuniversitycushingwhitneymedicallibrary bookleafnumber:556 bookleafnumber556 bookcollection:medicalheritagelibrary bookcollectionmedicalheritagelibrary bookcollection:cushingwhitneymedicallibrary bookcollectioncushingwhitneymedicallibrary bookcollection:americana bookcollectionamericana drawing surreal monochrome bookid:39002087820487.med.yale.edu bookid39002087820487medyaleedu bookyear:1914 bookyear1914 bookdecade:1910 bookdecade1910 bookcentury:1900 bookcentury1900 bookauthor:allen__carroll_woolsey_1874_ bookauthorallencarrollwoolsey1874 bookauthor:matas__rudolph_1860_1957 bookauthormatasrudolph18601957 booksubject:local_anesthetics booksubjectlocalanesthetics booksubject:anesthetics__local booksubjectanestheticslocal booksubject:anesthesia__local booksubjectanesthesialocal bookpublisher:philadelphia___w_b__saunders_co_ bookpublisherphiladelphiawbsaundersco bookcontributor:yale_university__cushing_whitney_medical_library bookcontributoryaleuniversitycushingwhitneymedicallibrary booksponsor:open_knowledge_commons_and_yale_university__cushing_whitney_medical_library booksponsoropenknowledgecommonsandyaleuniversitycushingwhitneymedicallibrary bookleafnumber:556 bookleafnumber556 bookcollection:medicalheritagelibrary bookcollectionmedicalheritagelibrary bookcollection:cushingwhitneymedicallibrary bookcollectioncushingwhitneymedicallibrary bookcollection:americana bookcollectionamericana drawing surreal monochrome bookid:39002087820487.med.yale.edu bookid39002087820487medyaleedu bookyear:1914 bookyear1914 bookdecade:1910 bookdecade1910 bookcentury:1900 bookcentury1900 bookauthor:allen__carroll_woolsey_1874_ bookauthorallencarrollwoolsey1874 bookauthor:matas__rudolph_1860_1957 bookauthormatasrudolph18601957 booksubject:local_anesthetics booksubjectlocalanesthetics booksubject:anesthetics__local booksubjectanestheticslocal booksubject:anesthesia__local booksubjectanesthesialocal bookpublisher:philadelphia___w_b__saunders_co_ bookpublisherphiladelphiawbsaundersco bookcontributor:yale_university__cushing_whitney_medical_library bookcontributoryaleuniversitycushingwhitneymedicallibrary booksponsor:open_knowledge_commons_and_yale_university__cushing_whitney_medical_library booksponsoropenknowledgecommonsandyaleuniversitycushingwhitneymedicallibrary bookleafnumber:556 bookleafnumber556 bookcollection:medicalheritagelibrary bookcollectionmedicalheritagelibrary bookcollection:cushingwhitneymedicallibrary bookcollectioncushingwhitneymedicallibrary bookcollection:americana bookcollectionamericana drawing surreal monochrome bookid:39002087820487.med.yale.edu bookid39002087820487medyaleedu bookyear:1914 bookyear1914 bookdecade:1910 bookdecade1910 bookcentury:1900 bookcentury1900 bookauthor:allen__carroll_woolsey_1874_ bookauthorallencarrollwoolsey1874 bookauthor:matas__rudolph_1860_1957 bookauthormatasrudolph18601957 booksubject:local_anesthetics booksubjectlocalanesthetics booksubject:anesthetics__local booksubjectanestheticslocal booksubject:anesthesia__local booksubjectanesthesialocal bookpublisher:philadelphia___w_b__saunders_co_ bookpublisherphiladelphiawbsaundersco bookcontributor:yale_university__cushing_whitney_medical_library bookcontributoryaleuniversitycushingwhitneymedicallibrary booksponsor:open_knowledge_commons_and_yale_university__cushing_whitney_medical_library booksponsoropenknowledgecommonsandyaleuniversitycushingwhitneymedicallibrary bookleafnumber:556 bookleafnumber556 bookcollection:medicalheritagelibrary bookcollectionmedicalheritagelibrary bookcollection:cushingwhitneymedicallibrary bookcollectioncushingwhitneymedicallibrary bookcollection:americana bookcollectionamericana drawing surreal monochrome Identifier: 39002087820487.med.yale.edu Title: Local and regional anesthesia : with chapters on spinal, epidural, paravertebral, and parasacral analgesia, and on other applications of local and regional anesthesia to the surgery of the eye, ear, nose and throat, and to dental practice Year: 1914 (1910s) Authors: Allen, Carroll Woolsey,1874- Matas, Rudolph,1860-1957 Subjects: Local anesthetics Anesthetics, Local Anesthesia, Local Publisher: Philadelphia : W.B. Saunders Co. Contributing Library: Yale University, Cushing/Whitney Medical Library Digitizing Sponsor: Open Knowledge Commons and Yale University, Cushing/Whitney Medical Library View Book Page: Book Viewer About This Book: Catalog Entry View All Images: All Images From Book Click here to view book online to see this illustration in context in a browseable online version of this book. Text Appearing Before Image: e, lower jaw, with pro-cessus coronoideus and temporal muscle (laterally) on the otherside, through into the fossa infratemporalis, and now endeavors byperforation of the pterygoideus muscle externus, which fills the entirefossa, to reach the planum infratemporale, in connection with which,as we have seen above, finger-feeling can be auxiliary only in a portionof the cases. We need, therefore, other fixed points. Such a point is THE HEAD, SCALP, CRANIUM. BRAIN, AND FACE 549 the depth. Before we stick the needle in we mark with the slidingcatch a distance of 5 to 6 cm.; in case of forward curving of the cheekby a tumor, still more. We are thereby always informed as to the depthreached, and can thus protect ourselves from gross errors. In thesecond place we must now consider a direction discernible on inspec-tion of the whole skull, and we have been able by careful observationand many examinations to establish as essential for the puncture ofthe foramen ovale the following fixed points: Text Appearing After Image: Fig. 216.—Lateral route to foramen rotundum. (Braun.) (1) Viewed exactly from the front (for this determination ofdirection one must, like the designer, see with one eye only, and possiblywith the aid of a second cannula held freely before one), the cannulaintroduced into the ganglion points to the pupil of the eye on thesame side (Fig. 205). If we observe this rule, then we avoid deviat-ing outwardly into the fossa temporalis, inwardly into the tube andpharynx region. (2) On exact lateral inspection the cannula points to the tuber- 55° LOCAL ANESTHESIA culum articulare of the zygomatic arch (Fig. 205), If we do not ob-serve this rule, then it may happen that we come too far forward intothe fossa pterygopalatina, or too far back into the region of the fora-men caroticum and of the foramen jugulare; the latter way, particu-larly—namely, the introduction of the needle into the medial partof the foramen jugulare instead of into the foramen ovale—we haveseveral times taken wrongly Note About Images Please note that these images are extracted from scanned page images that may have been digitally enhanced for readability - coloration and appearance of these illustrations may not perfectly resemble the original work. Identifier: 39002087820487.med.yale.edu Title: Local and regional anesthesia : with chapters on spinal, epidural, paravertebral, and parasacral analgesia, and on other applications of local and regional anesthesia to the surgery of the eye, ear, nose and throat, and to dental practice Year: 1914 (1910s) Authors: Allen, Carroll Woolsey,1874- Matas, Rudolph,1860-1957 Subjects: Local anesthetics Anesthetics, Local Anesthesia, Local Publisher: Philadelphia : W.B. Saunders Co. Contributing Library: Yale University, Cushing/Whitney Medical Library Digitizing Sponsor: Open Knowledge Commons and Yale University, Cushing/Whitney Medical Library View Book Page: Book Viewer About This Book: Catalog Entry View All Images: All Images From Book Click here to view book online to see this illustration in context in a browseable online version of this book. Text Appearing Before Image: e, lower jaw, with pro-cessus coronoideus and temporal muscle (laterally) on the otherside, through into the fossa infratemporalis, and now endeavors byperforation of the pterygoideus muscle externus, which fills the entirefossa, to reach the planum infratemporale, in connection with which,as we have seen above, finger-feeling can be auxiliary only in a portionof the cases. We need, therefore, other fixed points. Such a point is THE HEAD, SCALP, CRANIUM. BRAIN, AND FACE 549 the depth. Before we stick the needle in we mark with the slidingcatch a distance of 5 to 6 cm.; in case of forward curving of the cheekby a tumor, still more. We are thereby always informed as to the depthreached, and can thus protect ourselves from gross errors. In thesecond place we must now consider a direction discernible on inspec-tion of the whole skull, and we have been able by careful observationand many examinations to establish as essential for the puncture ofthe foramen ovale the following fixed points: Text Appearing After Image: Fig. 216.—Lateral route to foramen rotundum. (Braun.) (1) Viewed exactly from the front (for this determination ofdirection one must, like the designer, see with one eye only, and possiblywith the aid of a second cannula held freely before one), the cannulaintroduced into the ganglion points to the pupil of the eye on thesame side (Fig. 205). If we observe this rule, then we avoid deviat-ing outwardly into the fossa temporalis, inwardly into the tube andpharynx region. (2) On exact lateral inspection the cannula points to the tuber- 55° LOCAL ANESTHESIA culum articulare of the zygomatic arch (Fig. 205), If we do not ob-serve this rule, then it may happen that we come too far forward intothe fossa pterygopalatina, or too far back into the region of the fora-men caroticum and of the foramen jugulare; the latter way, particu-larly—namely, the introduction of the needle into the medial partof the foramen jugulare instead of into the foramen ovale—we haveseveral times taken wrongly Note About Images Please note that these images are extracted from scanned page images that may have been digitally enhanced for readability - coloration and appearance of these illustrations may not perfectly resemble the original work. Identifier: 39002087820487.med.yale.edu Title: Local and regional anesthesia : with chapters on spinal, epidural, paravertebral, and parasacral analgesia, and on other applications of local and regional anesthesia to the surgery of the eye, ear, nose and throat, and to dental practice Year: 1914 (1910s) Authors: Allen, Carroll Woolsey,1874- Matas, Rudolph,1860-1957 Subjects: Local anesthetics Anesthetics, Local Anesthesia, Local Publisher: Philadelphia : W.B. Saunders Co. Contributing Library: Yale University, Cushing/Whitney Medical Library Digitizing Sponsor: Open Knowledge Commons and Yale University, Cushing/Whitney Medical Library View Book Page: Book Viewer About This Book: Catalog Entry View All Images: All Images From Book Click here to view book online to see this illustration in context in a browseable online version of this book. Text Appearing Before Image: e, lower jaw, with pro-cessus coronoideus and temporal muscle (laterally) on the otherside, through into the fossa infratemporalis, and now endeavors byperforation of the pterygoideus muscle externus, which fills the entirefossa, to reach the planum infratemporale, in connection with which,as we have seen above, finger-feeling can be auxiliary only in a portionof the cases. We need, therefore, other fixed points. Such a point is THE HEAD, SCALP, CRANIUM. BRAIN, AND FACE 549 the depth. Before we stick the needle in we mark with the slidingcatch a distance of 5 to 6 cm.; in case of forward curving of the cheekby a tumor, still more. We are thereby always informed as to the depthreached, and can thus protect ourselves from gross errors. In thesecond place we must now consider a direction discernible on inspec-tion of the whole skull, and we have been able by careful observationand many examinations to establish as essential for the puncture ofthe foramen ovale the following fixed points: Text Appearing After Image: Fig. 216.—Lateral route to foramen rotundum. (Braun.) (1) Viewed exactly from the front (for this determination ofdirection one must, like the designer, see with one eye only, and possiblywith the aid of a second cannula held freely before one), the cannulaintroduced into the ganglion points to the pupil of the eye on thesame side (Fig. 205). If we observe this rule, then we avoid deviat-ing outwardly into the fossa temporalis, inwardly into the tube andpharynx region. (2) On exact lateral inspection the cannula points to the tuber- 55° LOCAL ANESTHESIA culum articulare of the zygomatic arch (Fig. 205), If we do not ob-serve this rule, then it may happen that we come too far forward intothe fossa pterygopalatina, or too far back into the region of the fora-men caroticum and of the foramen jugulare; the latter way, particu-larly—namely, the introduction of the needle into the medial partof the foramen jugulare instead of into the foramen ovale—we haveseveral times taken wrongly Note About Images Please note that these images are extracted from scanned page images that may have been digitally enhanced for readability - coloration and appearance of these illustrations may not perfectly resemble the original work. Identifier: 39002087820487.med.yale.edu Title: Local and regional anesthesia : with chapters on spinal, epidural, paravertebral, and parasacral analgesia, and on other applications of local and regional anesthesia to the surgery of the eye, ear, nose and throat, and to dental practice Year: 1914 (1910s) Authors: Allen, Carroll Woolsey,1874- Matas, Rudolph,1860-1957 Subjects: Local anesthetics Anesthetics, Local Anesthesia, Local Publisher: Philadelphia : W.B. Saunders Co. Contributing Library: Yale University, Cushing/Whitney Medical Library Digitizing Sponsor: Open Knowledge Commons and Yale University, Cushing/Whitney Medical Library View Book Page: Book Viewer About This Book: Catalog Entry View All Images: All Images From Book Click here to view book online to see this illustration in context in a browseable online version of this book. Text Appearing Before Image: e, lower jaw, with pro-cessus coronoideus and temporal muscle (laterally) on the otherside, through into the fossa infratemporalis, and now endeavors byperforation of the pterygoideus muscle externus, which fills the entirefossa, to reach the planum infratemporale, in connection with which,as we have seen above, finger-feeling can be auxiliary only in a portionof the cases. We need, therefore, other fixed points. Such a point is THE HEAD, SCALP, CRANIUM. BRAIN, AND FACE 549 the depth. Before we stick the needle in we mark with the slidingcatch a distance of 5 to 6 cm.; in case of forward curving of the cheekby a tumor, still more. We are thereby always informed as to the depthreached, and can thus protect ourselves from gross errors. In thesecond place we must now consider a direction discernible on inspec-tion of the whole skull, and we have been able by careful observationand many examinations to establish as essential for the puncture ofthe foramen ovale the following fixed points: Text Appearing After Image: Fig. 216.—Lateral route to foramen rotundum. (Braun.) (1) Viewed exactly from the front (for this determination ofdirection one must, like the designer, see with one eye only, and possiblywith the aid of a second cannula held freely before one), the cannulaintroduced into the ganglion points to the pupil of the eye on thesame side (Fig. 205). If we observe this rule, then we avoid deviat-ing outwardly into the fossa temporalis, inwardly into the tube andpharynx region. (2) On exact lateral inspection the cannula points to the tuber- 55° LOCAL ANESTHESIA culum articulare of the zygomatic arch (Fig. 205), If we do not ob-serve this rule, then it may happen that we come too far forward intothe fossa pterygopalatina, or too far back into the region of the fora-men caroticum and of the foramen jugulare; the latter way, particu-larly—namely, the introduction of the needle into the medial partof the foramen jugulare instead of into the foramen ovale—we haveseveral times taken wrongly Note About Images Please note that these images are extracted from scanned page images that may have been digitally enhanced for readability - coloration and appearance of these illustrations may not perfectly resemble the original work. Identifier: 39002087820487.med.yale.edu Title: Local and regional anesthesia : with chapters on spinal, epidural, paravertebral, and parasacral analgesia, and on other applications of local and regional anesthesia to the surgery of the eye, ear, nose and throat, and to dental practice Year: 1914 (1910s) Authors: Allen, Carroll Woolsey,1874- Matas, Rudolph,1860-1957 Subjects: Local anesthetics Anesthetics, Local Anesthesia, Local Publisher: Philadelphia : W.B. Saunders Co. Contributing Library: Yale University, Cushing/Whitney Medical Library Digitizing Sponsor: Open Knowledge Commons and Yale University, Cushing/Whitney Medical Library View Book Page: Book Viewer About This Book: Catalog Entry View All Images: All Images From Book Click here to view book online to see this illustration in context in a browseable online version of this book. Text Appearing Before Image: e, lower jaw, with pro-cessus coronoideus and temporal muscle (laterally) on the otherside, through into the fossa infratemporalis, and now endeavors byperforation of the pterygoideus muscle externus, which fills the entirefossa, to reach the planum infratemporale, in connection with which,as we have seen above, finger-feeling can be auxiliary only in a portionof the cases. We need, therefore, other fixed points. Such a point is THE HEAD, SCALP, CRANIUM. BRAIN, AND FACE 549 the depth. Before we stick the needle in we mark with the slidingcatch a distance of 5 to 6 cm.; in case of forward curving of the cheekby a tumor, still more. We are thereby always informed as to the depthreached, and can thus protect ourselves from gross errors. In thesecond place we must now consider a direction discernible on inspec-tion of the whole skull, and we have been able by careful observationand many examinations to establish as essential for the puncture ofthe foramen ovale the following fixed points: Text Appearing After Image: Fig. 216.—Lateral route to foramen rotundum. (Braun.) (1) Viewed exactly from the front (for this determination ofdirection one must, like the designer, see with one eye only, and possiblywith the aid of a second cannula held freely before one), the cannulaintroduced into the ganglion points to the pupil of the eye on thesame side (Fig. 205). If we observe this rule, then we avoid deviat-ing outwardly into the fossa temporalis, inwardly into the tube andpharynx region. (2) On exact lateral inspection the cannula points to the tuber- 55° LOCAL ANESTHESIA culum articulare of the zygomatic arch (Fig. 205), If we do not ob-serve this rule, then it may happen that we come too far forward intothe fossa pterygopalatina, or too far back into the region of the fora-men caroticum and of the foramen jugulare; the latter way, particu-larly—namely, the introduction of the needle into the medial partof the foramen jugulare instead of into the foramen ovale—we haveseveral times taken wrongly Note About Images Please note that these images are extracted from scanned page images that may have been digitally enhanced for readability - coloration and appearance of these illustrations may not perfectly resemble the original work. Identifier: 39002087820487.med.yale.edu Title: Local and regional anesthesia : with chapters on spinal, epidural, paravertebral, and parasacral analgesia, and on other applications of local and regional anesthesia to the surgery of the eye, ear, nose and throat, and to dental practice Year: 1914 (1910s) Authors: Allen, Carroll Woolsey,1874- Matas, Rudolph,1860-1957 Subjects: Local anesthetics Anesthetics, Local Anesthesia, Local Publisher: Philadelphia : W.B. Saunders Co. Contributing Library: Yale University, Cushing/Whitney Medical Library Digitizing Sponsor: Open Knowledge Commons and Yale University, Cushing/Whitney Medical Library View Book Page: Book Viewer About This Book: Catalog Entry View All Images: All Images From Book Click here to view book online to see this illustration in context in a browseable online version of this book. Text Appearing Before Image: e, lower jaw, with pro-cessus coronoideus and temporal muscle (laterally) on the otherside, through into the fossa infratemporalis, and now endeavors byperforation of the pterygoideus muscle externus, which fills the entirefossa, to reach the planum infratemporale, in connection with which,as we have seen above, finger-feeling can be auxiliary only in a portionof the cases. We need, therefore, other fixed points. Such a point is THE HEAD, SCALP, CRANIUM. BRAIN, AND FACE 549 the depth. Before we stick the needle in we mark with the slidingcatch a distance of 5 to 6 cm.; in case of forward curving of the cheekby a tumor, still more. We are thereby always informed as to the depthreached, and can thus protect ourselves from gross errors. In thesecond place we must now consider a direction discernible on inspec-tion of the whole skull, and we have been able by careful observationand many examinations to establish as essential for the puncture ofthe foramen ovale the following fixed points: Text Appearing After Image: Fig. 216.—Lateral route to foramen rotundum. (Braun.) (1) Viewed exactly from the front (for this determination ofdirection one must, like the designer, see with one eye only, and possiblywith the aid of a second cannula held freely before one), the cannulaintroduced into the ganglion points to the pupil of the eye on thesame side (Fig. 205). If we observe this rule, then we avoid deviat-ing outwardly into the fossa temporalis, inwardly into the tube andpharynx region. (2) On exact lateral inspection the cannula points to the tuber- 55° LOCAL ANESTHESIA culum articulare of the zygomatic arch (Fig. 205), If we do not ob-serve this rule, then it may happen that we come too far forward intothe fossa pterygopalatina, or too far back into the region of the fora-men caroticum and of the foramen jugulare; the latter way, particu-larly—namely, the introduction of the needle into the medial partof the foramen jugulare instead of into the foramen ovale—we haveseveral times taken wrongly Note About Images Please note that these images are extracted from scanned page images that may have been digitally enhanced for readability - coloration and appearance of these illustrations may not perfectly resemble the original work. Identifier: 39002087820487.med.yale.edu Title: Local and regional anesthesia : with chapters on spinal, epidural, paravertebral, and parasacral analgesia, and on other applications of local and regional anesthesia to the surgery of the eye, ear, nose and throat, and to dental practice Year: 1914 (1910s) Authors: Allen, Carroll Woolsey,1874- Matas, Rudolph,1860-1957 Subjects: Local anesthetics Anesthetics, Local Anesthesia, Local Publisher: Philadelphia : W.B. Saunders Co. Contributing Library: Yale University, Cushing/Whitney Medical Library Digitizing Sponsor: Open Knowledge Commons and Yale University, Cushing/Whitney Medical Library View Book Page: Book Viewer About This Book: Catalog Entry View All Images: All Images From Book Click here to view book online to see this illustration in context in a browseable online version of this book. Text Appearing Before Image: e, lower jaw, with pro-cessus coronoideus and temporal muscle (laterally) on the otherside, through into the fossa infratemporalis, and now endeavors byperforation of the pterygoideus muscle externus, which fills the entirefossa, to reach the planum infratemporale, in connection with which,as we have seen above, finger-feeling can be auxiliary only in a portionof the cases. We need, therefore, other fixed points. Such a point is THE HEAD, SCALP, CRANIUM. BRAIN, AND FACE 549 the depth. Before we stick the needle in we mark with the slidingcatch a distance of 5 to 6 cm.; in case of forward curving of the cheekby a tumor, still more. We are thereby always informed as to the depthreached, and can thus protect ourselves from gross errors. In thesecond place we must now consider a direction discernible on inspec-tion of the whole skull, and we have been able by careful observationand many examinations to establish as essential for the puncture ofthe foramen ovale the following fixed points: Text Appearing After Image: Fig. 216.—Lateral route to foramen rotundum. (Braun.) (1) Viewed exactly from the front (for this determination ofdirection one must, like the designer, see with one eye only, and possiblywith the aid of a second cannula held freely before one), the cannulaintroduced into the ganglion points to the pupil of the eye on thesame side (Fig. 205). If we observe this rule, then we avoid deviat-ing outwardly into the fossa temporalis, inwardly into the tube andpharynx region. (2) On exact lateral inspection the cannula points to the tuber- 55° LOCAL ANESTHESIA culum articulare of the zygomatic arch (Fig. 205), If we do not ob-serve this rule, then it may happen that we come too far forward intothe fossa pterygopalatina, or too far back into the region of the fora-men caroticum and of the foramen jugulare; the latter way, particu-larly—namely, the introduction of the needle into the medial partof the foramen jugulare instead of into the foramen ovale—we haveseveral times taken wrongly Note About Images Please note that these images are extracted from scanned page images that may have been digitally enhanced for readability - coloration and appearance of these illustrations may not perfectly resemble the original work. Identifier: 39002087820487.med.yale.edu Title: Local and regional anesthesia : with chapters on spinal, epidural, paravertebral, and parasacral analgesia, and on other applications of local and regional anesthesia to the surgery of the eye, ear, nose and throat, and to dental practice Year: 1914 (1910s) Authors: Allen, Carroll Woolsey,1874- Matas, Rudolph,1860-1957 Subjects: Local anesthetics Anesthetics, Local Anesthesia, Local Publisher: Philadelphia : W.B. Saunders Co. Contributing Library: Yale University, Cushing/Whitney Medical Library Digitizing Sponsor: Open Knowledge Commons and Yale University, Cushing/Whitney Medical Library View Book Page: Book Viewer About This Book: Catalog Entry View All Images: All Images From Book Click here to view book online to see this illustration in context in a browseable online version of this book. Text Appearing Before Image: e, lower jaw, with pro-cessus coronoideus and temporal muscle (laterally) on the otherside, through into the fossa infratemporalis, and now endeavors byperforation of the pterygoideus muscle externus, which fills the entirefossa, to reach the planum infratemporale, in connection with which,as we have seen above, finger-feeling can be auxiliary only in a portionof the cases. We need, therefore, other fixed points. Such a point is THE HEAD, SCALP, CRANIUM. BRAIN, AND FACE 549 the depth. Before we stick the needle in we mark with the slidingcatch a distance of 5 to 6 cm.; in case of forward curving of the cheekby a tumor, still more. We are thereby always informed as to the depthreached, and can thus protect ourselves from gross errors. In thesecond place we must now consider a direction discernible on inspec-tion of the whole skull, and we have been able by careful observationand many examinations to establish as essential for the puncture ofthe foramen ovale the following fixed points: Text Appearing After Image: Fig. 216.—Lateral route to foramen rotundum. (Braun.) (1) Viewed exactly from the front (for this determination ofdirection one must, like the designer, see with one eye only, and possiblywith the aid of a second cannula held freely before one), the cannulaintroduced into the ganglion points to the pupil of the eye on thesame side (Fig. 205). If we observe this rule, then we avoid deviat-ing outwardly into the fossa temporalis, inwardly into the tube andpharynx region. (2) On exact lateral inspection the cannula points to the tuber- 55° LOCAL ANESTHESIA culum articulare of the zygomatic arch (Fig. 205), If we do not ob-serve this rule, then it may happen that we come too far forward intothe fossa pterygopalatina, or too far back into the region of the fora-men caroticum and of the foramen jugulare; the latter way, particu-larly—namely, the introduction of the needle into the medial partof the foramen jugulare instead of into the foramen ovale—we haveseveral times taken wrongly Note About Images Please note that these images are extracted from scanned page images that may have been digitally enhanced for readability - coloration and appearance of these illustrations may not perfectly resemble the original work. Identifier: 39002087820487.med.yale.edu Title: Local and regional anesthesia : with chapters on spinal, epidural, paravertebral, and parasacral analgesia, and on other applications of local and regional anesthesia to the surgery of the eye, ear, nose and throat, and to dental practice Year: 1914 (1910s) Authors: Allen, Carroll Woolsey,1874- Matas, Rudolph,1860-1957 Subjects: Local anesthetics Anesthetics, Local Anesthesia, Local Publisher: Philadelphia : W.B. Saunders Co. Contributing Library: Yale University, Cushing/Whitney Medical Library Digitizing Sponsor: Open Knowledge Commons and Yale University, Cushing/Whitney Medical Library View Book Page: Book Viewer About This Book: Catalog Entry View All Images: All Images From Book Click here to view book online to see this illustration in context in a browseable online version of this book. Text Appearing Before Image: e, lower jaw, with pro-cessus coronoideus and temporal muscle (laterally) on the otherside, through into the fossa infratemporalis, and now endeavors byperforation of the pterygoideus muscle externus, which fills the entirefossa, to reach the planum infratemporale, in connection with which,as we have seen above, finger-feeling can be auxiliary only in a portionof the cases. We need, therefore, other fixed points. Such a point is THE HEAD, SCALP, CRANIUM. BRAIN, AND FACE 549 the depth. Before we stick the needle in we mark with the slidingcatch a distance of 5 to 6 cm.; in case of forward curving of the cheekby a tumor, still more. We are thereby always informed as to the depthreached, and can thus protect ourselves from gross errors. In thesecond place we must now consider a direction discernible on inspec-tion of the whole skull, and we have been able by careful observationand many examinations to establish as essential for the puncture ofthe foramen ovale the following fixed points: Text Appearing After Image: Fig. 216.—Lateral route to foramen rotundum. (Braun.) (1) Viewed exactly from the front (for this determination ofdirection one must, like the designer, see with one eye only, and possiblywith the aid of a second cannula held freely before one), the cannulaintroduced into the ganglion points to the pupil of the eye on thesame side (Fig. 205). If we observe this rule, then we avoid deviat-ing outwardly into the fossa temporalis, inwardly into the tube andpharynx region. (2) On exact lateral inspection the cannula points to the tuber- 55° LOCAL ANESTHESIA culum articulare of the zygomatic arch (Fig. 205), If we do not ob-serve this rule, then it may happen that we come too far forward intothe fossa pterygopalatina, or too far back into the region of the fora-men caroticum and of the foramen jugulare; the latter way, particu-larly—namely, the introduction of the needle into the medial partof the foramen jugulare instead of into the foramen ovale—we haveseveral times taken wrongly Note About Images Please note that these images are extracted from scanned page images that may have been digitally enhanced for readability - coloration and appearance of these illustrations may not perfectly resemble the original work. Identifier: 39002087820487.med.yale.edu Title: Local and regional anesthesia : with chapters on spinal, epidural, paravertebral, and parasacral analgesia, and on other applications of local and regional anesthesia to the surgery of the eye, ear, nose and throat, and to dental practice Year: 1914 (1910s) Authors: Allen, Carroll Woolsey,1874- Matas, Rudolph,1860-1957 Subjects: Local anesthetics Anesthetics, Local Anesthesia, Local Publisher: Philadelphia : W.B. Saunders Co. Contributing Library: Yale University, Cushing/Whitney Medical Library Digitizing Sponsor: Open Knowledge Commons and Yale University, Cushing/Whitney Medical Library View Book Page: Book Viewer About This Book: Catalog Entry View All Images: All Images From Book Click here to view book online to see this illustration in context in a browseable online version of this book. Text Appearing Before Image: e, lower jaw, with pro-cessus coronoideus and temporal muscle (laterally) on the otherside, through into the fossa infratemporalis, and now endeavors byperforation of the pterygoideus muscle externus, which fills the entirefossa, to reach the planum infratemporale, in connection with which,as we have seen above, finger-feeling can be auxiliary only in a portionof the cases. We need, therefore, other fixed points. Such a point is THE HEAD, SCALP, CRANIUM. BRAIN, AND FACE 549 the depth. Before we stick the needle in we mark with the slidingcatch a distance of 5 to 6 cm.; in case of forward curving of the cheekby a tumor, still more. We are thereby always informed as to the depthreached, and can thus protect ourselves from gross errors. In thesecond place we must now consider a direction discernible on inspec-tion of the whole skull, and we have been able by careful observationand many examinations to establish as essential for the puncture ofthe foramen ovale the following fixed points: Text Appearing After Image: Fig. 216.—Lateral route to foramen rotundum. (Braun.) (1) Viewed exactly from the front (for this determination ofdirection one must, like the designer, see with one eye only, and possiblywith the aid of a second cannula held freely before one), the cannulaintroduced into the ganglion points to the pupil of the eye on thesame side (Fig. 205). If we observe this rule, then we avoid deviat-ing outwardly into the fossa temporalis, inwardly into the tube andpharynx region. (2) On exact lateral inspection the cannula points to the tuber- 55° LOCAL ANESTHESIA culum articulare of the zygomatic arch (Fig. 205), If we do not ob-serve this rule, then it may happen that we come too far forward intothe fossa pterygopalatina, or too far back into the region of the fora-men caroticum and of the foramen jugulare; the latter way, particu-larly—namely, the introduction of the needle into the medial partof the foramen jugulare instead of into the foramen ovale—we haveseveral times taken wrongly Note About Images Please note that these images are extracted from scanned page images that may have been digitally enhanced for readability - coloration and appearance of these illustrations may not perfectly resemble the original work. Identifier: 39002087820487.med.yale.edu Title: Local and regional anesthesia : with chapters on spinal, epidural, paravertebral, and parasacral analgesia, and on other applications of local and regional anesthesia to the surgery of the eye, ear, nose and throat, and to dental practice Year: 1914 (1910s) Authors: Allen, Carroll Woolsey,1874- Matas, Rudolph,1860-1957 Subjects: Local anesthetics Anesthetics, Local Anesthesia, Local Publisher: Philadelphia : W.B. Saunders Co. Contributing Library: Yale University, Cushing/Whitney Medical Library Digitizing Sponsor: Open Knowledge Commons and Yale University, Cushing/Whitney Medical Library View Book Page: Book Viewer About This Book: Catalog Entry View All Images: All Images From Book Click here to view book online to see this illustration in context in a browseable online version of this book. Text Appearing Before Image: e, lower jaw, with pro-cessus coronoideus and temporal muscle (laterally) on the otherside, through into the fossa infratemporalis, and now endeavors byperforation of the pterygoideus muscle externus, which fills the entirefossa, to reach the planum infratemporale, in connection with which,as we have seen above, finger-feeling can be auxiliary only in a portionof the cases. We need, therefore, other fixed points. Such a point is THE HEAD, SCALP, CRANIUM. BRAIN, AND FACE 549 the depth. Before we stick the needle in we mark with the slidingcatch a distance of 5 to 6 cm.; in case of forward curving of the cheekby a tumor, still more. We are thereby always informed as to the depthreached, and can thus protect ourselves from gross errors. In thesecond place we must now consider a direction discernible on inspec-tion of the whole skull, and we have been able by careful observationand many examinations to establish as essential for the puncture ofthe foramen ovale the following fixed points: Text Appearing After Image: Fig. 216.—Lateral route to foramen rotundum. (Braun.) (1) Viewed exactly from the front (for this determination ofdirection one must, like the designer, see with one eye only, and possiblywith the aid of a second cannula held freely before one), the cannulaintroduced into the ganglion points to the pupil of the eye on thesame side (Fig. 205). If we observe this rule, then we avoid deviat-ing outwardly into the fossa temporalis, inwardly into the tube andpharynx region. (2) On exact lateral inspection the cannula points to the tuber- 55° LOCAL ANESTHESIA culum articulare of the zygomatic arch (Fig. 205), If we do not ob-serve this rule, then it may happen that we come too far forward intothe fossa pterygopalatina, or too far back into the region of the fora-men caroticum and of the foramen jugulare; the latter way, particu-larly—namely, the introduction of the needle into the medial partof the foramen jugulare instead of into the foramen ovale—we haveseveral times taken wrongly Note About Images Please note that these images are extracted from scanned page images that may have been digitally enhanced for readability - coloration and appearance of these illustrations may not perfectly resemble the original work. Identifier: 39002087820487.med.yale.edu Title: Local and regional anesthesia : with chapters on spinal, epidural, paravertebral, and parasacral analgesia, and on other applications of local and regional anesthesia to the surgery of the eye, ear, nose and throat, and to dental practice Year: 1914 (1910s) Authors: Allen, Carroll Woolsey,1874- Matas, Rudolph,1860-1957 Subjects: Local anesthetics Anesthetics, Local Anesthesia, Local Publisher: Philadelphia : W.B. Saunders Co. Contributing Library: Yale University, Cushing/Whitney Medical Library Digitizing Sponsor: Open Knowledge Commons and Yale University, Cushing/Whitney Medical Library View Book Page: Book Viewer About This Book: Catalog Entry View All Images: All Images From Book Click here to view book online to see this illustration in context in a browseable online version of this book. Text Appearing Before Image: e, lower jaw, with pro-cessus coronoideus and temporal muscle (laterally) on the otherside, through into the fossa infratemporalis, and now endeavors byperforation of the pterygoideus muscle externus, which fills the entirefossa, to reach the planum infratemporale, in connection with which,as we have seen above, finger-feeling can be auxiliary only in a portionof the cases. We need, therefore, other fixed points. Such a point is THE HEAD, SCALP, CRANIUM. BRAIN, AND FACE 549 the depth. Before we stick the needle in we mark with the slidingcatch a distance of 5 to 6 cm.; in case of forward curving of the cheekby a tumor, still more. We are thereby always informed as to the depthreached, and can thus protect ourselves from gross errors. In thesecond place we must now consider a direction discernible on inspec-tion of the whole skull, and we have been able by careful observationand many examinations to establish as essential for the puncture ofthe foramen ovale the following fixed points: Text Appearing After Image: Fig. 216.—Lateral route to foramen rotundum. (Braun.) (1) Viewed exactly from the front (for this determination ofdirection one must, like the designer, see with one eye only, and possiblywith the aid of a second cannula held freely before one), the cannulaintroduced into the ganglion points to the pupil of the eye on thesame side (Fig. 205). If we observe this rule, then we avoid deviat-ing outwardly into the fossa temporalis, inwardly into the tube andpharynx region. (2) On exact lateral inspection the cannula points to the tuber- 55° LOCAL ANESTHESIA culum articulare of the zygomatic arch (Fig. 205), If we do not ob-serve this rule, then it may happen that we come too far forward intothe fossa pterygopalatina, or too far back into the region of the fora-men caroticum and of the foramen jugulare; the latter way, particu-larly—namely, the introduction of the needle into the medial partof the foramen jugulare instead of into the foramen ovale—we haveseveral times taken wrongly Note About Images Please note that these images are extracted from scanned page images that may have been digitally enhanced for readability - coloration and appearance of these illustrations may not perfectly resemble the original work. | ||||
{kind=link}